We have recently noticed several facilities that have used their fire alarm zones as part of their evacuation plan. The fire alarm zones are the zones on the fire alarm panel used to help staff identify the location of the fire. These are different from smoke zones, which are the zones in the building created to prevent the spread of smoke and fire and allow staff time to complete a full evacuation of the building. Many facilities have fire alarm zones that do not match the smoke zones in the facility. Often times there are more fire zones to help staff identify the location of a fire.
To start a smoke zone evacuation, it may be necessary to evacuate multiple fire alarm zones at the same time. The evacuation plans need to have these smoke zones clearly labeled and all staff need to know where they will move the residents in the event of a fire. The facility cannot base their evacuation plans on the fire alarm zones.
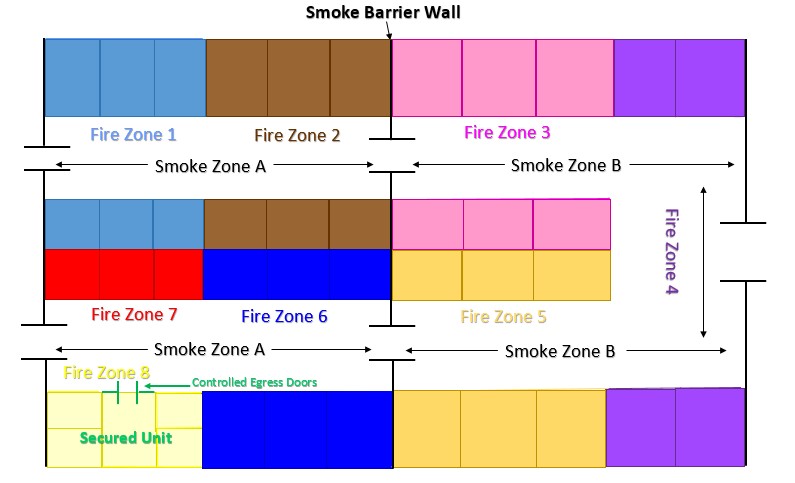
In this example, the facility has eight fire alarm zones (Fire Zones 1-8). The facility has a smoke barrier wall that divides the facility into two smoke zones (Smoke Zones A and B). The facility also has a secured unit, but the controlled egress doors (locked keypad doors) are not a part of the smoke barrier wall, so the secured unit is part of Smoke Zone A.
If a fire occurs in Fire Zone 4, it means that an evacuation of all residents would need to occur throughout Smoke Zone B, which would include all residents in Fire Zones 3, 4, and 5. The evacuation plan may mention things like room number, dining rooms, etc., but should avoid using fire zones to describe the smoke zones. Although it is important to know which smoke zone activated the fire alarm system, staff cannot move the residents from Fire Zone 4 to Fire Zone 5, as they are still within Smoke Zone B. Staff must completely move the residents out of Smoke Zone B.
In addition, it is significant to note if a fire occurred in Smoke Zone A (i.e. Fire Zones 1 or 6), the staff would need to move residents in the secured unit from Smoke Zone A. Staff cannot leave the residents in the secured unit since a smoke barrier wall does not protect the secured unit and it is not its own smoke zone.
The facility must have the evacuation plans posted on at least every floor of the facility [19 CSR 30-85.022 (33)(B)(2)] which directs all staff, residents, and visitors where to go in the event of a facility evacuation. The policy and procedure for evacuations also needs to be in the emergency preparedness manual.
NFPA 99, 2012 edition
15.7.4.3.1: Where buildings are required to be subdivided into smoke compartments, fire alarm notification zones shall coincide with one or more smoke compartment boundaries or shall be in accordance with the facility fire plan.
